


28/08/2018 0 Σχόλια
Dens invaginatus in a mandibular lateral incisor
Dens invaginatus in a mandibular lateral incisor
M. G. KHABBAZ, M. KONSTANTAK1 & S. N. SYKARAS
Department of Endodontics. University of Athens, School of Dentistry. Athens, Greece
Summary
A rare case of dens invaginatus involving a non-carious mandibular lateral incisor with periapical periodontitis is reported. Invaginated teeth present technical difficulties in their clinical management because of their abnormal anatomy. In the present case, non-surgical root canal therapy was chosen. A one-year follow-up clinical and radiographic examination showed a non-symptomatic tooth with osseous healing proceeding.
A rare case of dens invaginatus involving a non-carious mandibular lateral incisor with periapical periodontitis is reported. Invaginated teeth present technical difficulties in their clinical management because of their abnormal anatomy. In the present case, non-surgical root canal therapy was chosen. A one-year follow-up clinical and radiographic examination showed a non-symptomatic tooth with osseous healing proceeding.
Keywords: dens in dente, dens invaginatus, tooth abnormality
Introduction
There are many reports in the dental literature concerning abnormalities such as gemination, fusion and dens invaginatus (Oehlers 1957. Pindborg 1970. Burzynski 1973. Hovland & Block 1977. Shifman & Tamir 1979, Szajkis & Kaufman 1993, Benenati 1994). Dens Invoginatas occurs more commonly in the maxillary permanent lateral incisors than in central incisors, premolars, canines and molars. The reported incidence for dens invaginatus ranges from 0.04 to 10% (Hovland & Block 1977). and is very rare in the mandible and in the primary dentition (Pindborg 1970). but recent reports have shown involvement of mandibular premolars (Eldeeb 1984, Tavano et al. 1994).
According to Oehlers (1957), dens invaginatus may have three forms: (1) an enamel-lined minor type occurring within the crown of the tooth and not extending beyond the cementoenamel junction: (2) an enamel-lined type which invades the root as a blind sac and may connect with the dental pulp; and (3) a severe type which extends through the root and opens in the apical region without connection with the pulp. The purpose of this article is to report on the clinical management of a case of type 3 dens invaginatus involving the right mandibular lateral incisor, with a periapical lesion.
Case report
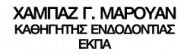
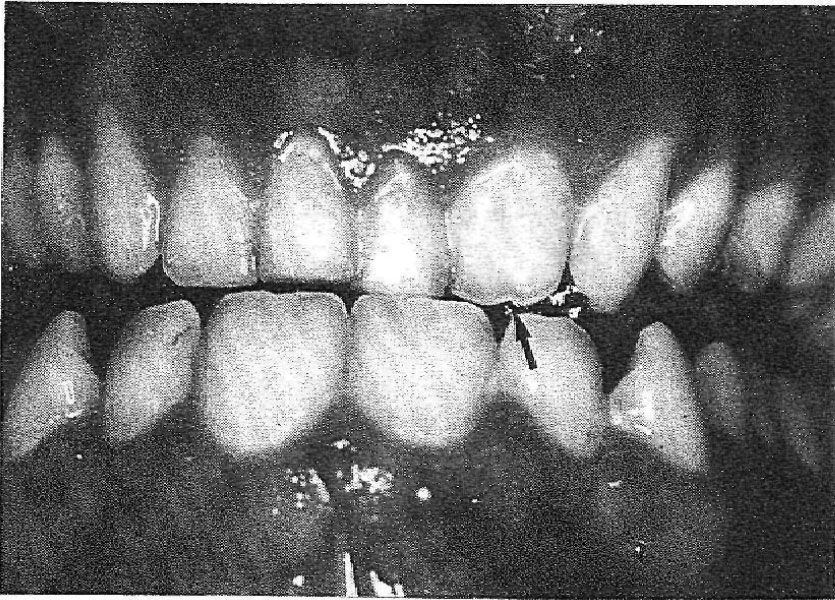
A 25-year-old Greek male complaining of acute pain in the right mandibular lateral incisor (42) was referred to the Endodontic Clinic at the University of Athens. The patient's medical and dental history was uncomplicated. The clinical examination showed that the tooth was tender to percussion and palpation, but free of decay, Pulp sensitivity tests (thermal and electrical) were negative. There was no history of trauma and the patient had no harmful habits. The crown of tooth 42 was wider than that of the left mandibular lateral incisor (32). In the labial surface of the crown, there was a groove, and in the lingual, a pit. The colour of the tooth did not differ from the adjacent teeth and the total number of teeth in the arch was normal (Figs 1 & 2). Radiographic examination revealed that the tooth had a single broad root with two separate root canals. ln the mescal pulp cavity, there was a dens invaginatus extending through the root and opening in the apical region. In the periapical region, there was a radiolucency (Fig. 3).
A diagnosis of acute periapical abscess was made and the tooth was opened for drainage. After 4 days, cleaning and shaping of root canals was performed with K files, using the step-back technique and 1-2 ml of 3% sodium hypochlorite irrigant after each file used.At the end of the appointment the root canals were dried and filled with calcium hydroxide paste and the access cavity dressed with a zinc-oxide eugenol cement.
The patient returned after 3 months, and canals were obturated with Grossman's sealer and gutta-percha using the lateral condensation technique in the distal canal and vertical condensation of warm gutta-percha in the mesial canal, the latter in an attempt to fill possible irregularities in this canal space. There did not appear to be any communication with the distal root canal (Fig. 4).
One year post-operatively, the patient remained asymptomatic and there was radiographic evidence or periapical healing (Fig. 5).
Discussion
The case reported in the present paper had a broad crown and root, and two separate pulp chambers leading into two separate root canals.
The case reported in the present paper had a broad crown and root, and two separate pulp chambers leading into two separate root canals.
The presence of an invaginated deep lingual pit in the mesial root canal renders the tooth susceptible to invasion by microorganisms, and subsequent pulpal Infection with necrosis and the development of peri-apical periodontitis. The fact that there was no obvious connection between the invaginated space and the main canal suggests that the pulp necrosis in the main canal occurred as a result of dentine permeability between the two canals. Some authors have reported similar cases in the maxilla. but these were characterized as fusion or gemination (Burzynski 1973, Shifman & Tamir 1979).
In spite of difficulties faced during the root canal treatment, such as diagnosis. access preparation, and clean¬ing and shaping, the patient’s recall examination demonstrated an asymptomatic tooth with evidence of healing of the periapical lesion. Similar reports on the successful conservative management of such tomes have been published (Morfis & Lentzari 1989. Vajrabhaya 1989).
For the references, click the file below:
Dens_invaginatus.pdf




Σχόλια