



28/08/2018 0 Σχόλια
Deposition of calcified tissue around an overextended gutta-percha cone: case report
Abstract
Root canal treatment was performed in a mandibular right second premolar with a periapical lesion and apical resorption. The root canal was prepared with K-files using the step-back technique and 3% NaOCl as an irrigant; during obturation gross overfilling of gutta-percha occurred. The tooth was permanently restored with a post and core along with a crown. Although healing of the periapical lesion occurred and the patient reported that he was symptom-free, the tooth was extracted after 4 years because of a subgingival root fracture. Following extraction the tooth was examined with SEM. The examination revealed the presence of newly formed calcified tissue at resorption sites on the root apex. This newly formed tissue extended from the surface of the root around the apex to the extruded gutta-percha cone to which it was well adapted, forming a bridge between the cone and the root.
Keywords: calcified tissues, root canal filling, root canal therapy, toxicity.
Introduction
The obturation of the root canal system is one of the most important factors in the success of root canal treatment. It is generally agreed that all root canal filling materials should be confined to the root canal space. However, in clinical endodontics, it is not uncommon for overfilling to occur, especially in cases of immature, resorbed or overinstrumented root canal apices. Although the success rate of root canal treatment varies between 85 and 95% (Kerekes & Tronstad 1979, Swartz et al. 1983), it is generally accepted that a higher failure rate is found in overin¬strumented and overfilled teeth (Bergenholtz et al. 1979, Swartz et al. 1983, Seltzer 1988).
Gutta-percha is the most widely used root canal filling material. It is considered to be the least toxic and is well tolerated by connective tissue (Kawahara et al. 1968, Wolfson & Seltzer 1975, Olsson & Wennberg1985). Nevertheless it has been demonstrated that the additives in the different brands of the commercially available gutta-percha cones account for varying degrees of toxicity (Holland et al. 1982, Leonardo et al. 1990, Tavares et al. 1994).
According to Seltzer et al. (1973), overinstrumenta¬tion and overfilling of teeth evoked persistent chronic inflammation with a tendency towards epithelial prolif-eration and cyst formation. It has also been demon¬strated that the extrusion of root canal cements in the periapical tissues produces inflammation and may cause necrosis of cementum, periodontal ligament and bone (Erausquin et al. 1966, Muruzabal et al. 1966, Erausquin & Muruzabal 1968). Nevertheless, in many clinical cases gutta-percha cones are extended into the periapical tissues for years in well obturated root canals without clinical or radiographic evidence of failure (Feldman et al. 1965, Weine 1996).
The purpose of this article is to report a case of a tooth with a periapical lesion and a root canal overfilled with gutta-percha where deposition of calcified tissue occurred at the apex.
Case report
The mandibular right second premolar (tooth 45) of a 37-year-old male received root canal treatment. Most of the crown of the tooth was lost because of gross caries and the patient was symptom-free. In the preo¬perative radiograph there was a radiolucent lesion associated with the apex of the premolar which appeared resorbed (Fig. 1).
The root canal was prepared with K-files using the step-back technique and 3% NaOC1 as an irrigant. Laterally condensed cold gutta-percha and Roth 811 (Roth International, Chicago IL, USA) root canal sealer were used for the obturation of the root canal. The post¬operative radiograph revealed an overfilling that extended 4-5 mm into the periapical tissues. Although an attempt was made to re-treat the case immediately, the overextended gutta-percha was unintentionally cut off and was pushed further into the periradicular tissues. In the final postoperative radiograph there was an overfilling of approximately 1 mm. After two recalls at 3 and 6 months, the patient remained symptomless and it was decided that the tooth could be permanently restored with a postcore and crown fixed restoration.
Four years later, the same patient returned with a subgingival root fracture involving the same premolar. The postcore and crown restorations were lost. During this period the patient reported that he was symptom-free, which was confirmed by clinical examination. In the radiographic examination, healing of the periradi¬cular tissues was apparent (Fig. 2). It was decided that the remaining root could not be restored and was extracted.
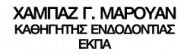
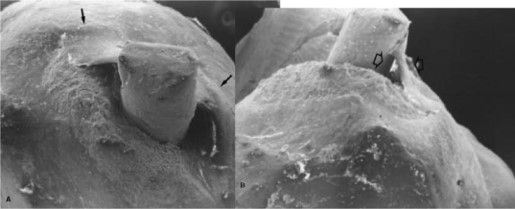
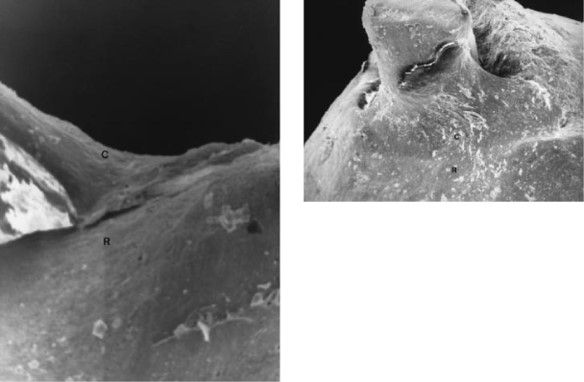
The SEM examination revealed the presence of calcified tissue extending from the surface of the root around the apex to the extruded gutta-percha cone, forming a bridge between them (Fig. 3). A clear contact line was noticed between the newly formed tissue and the apex (Fig. 4). The surface of this tissue was smooth and had a similar appearance to the surface of the cementum of the root to which it appeared to be tightly attached (Fig. 5). The formed tissue adapted closely to the extending gutta-percha but small voids were also observed. The remainder of the surface of the root around the apex had a rough appearance (Fig. 3).Despite 4-5 mm of gutta-percha that were pushed into the periradicular tissues and the fmal 1 min overfill, there was healing of the periradicular tissues 4 years after the completion of the root canal treatment and the patient remained asymptomatic. The case was considered successful according to the criteria for evaluating the success of endodontic therapy (Bender et al. 1966).
The healing of the periapical lesion in this case was attributed to the successful control of the infection through root canal preparation and debridement as well as the obturation of the root canal. This healing process was not affected by the presence of filling materials in the periradicular tissues, which is in agreement with studies that report gutta-percha to be well tolerated (Wolfson & Seltzer 1975, Olsson & Wennberg 1985).
In clinical endodontics, it is well established that the absence of irritants in the root canal and the periradi¬cular tissues creates favourable conditions for healing, i.e. bone deposition in the periapical lesions and hard tissue formation on the root surface around the apex together with the absence of clinical symptoms. (Seltzer 1988, Weine 1996).
In teeth of animals with induced periapical lesions, cementum deposition was apparent at the root apex 12 weeks after root canal treatment. This deposition was considered as early histological proof of healing (Fouad et al. 1993). Deposition of hard tissue has also been demonstrated histologically in the root canal space of overinstrumented and underfilled root canals in animals (Davis et al. 1971, Benatti et al. 1985). Ad-ditionally, in long-term follow-up radiographs of successful cases of root-canal-treated teeth with periapical lesions and apical resorption, cementum deposition is obvious at the root apex (Weine 1996). In the present case the SEM examination of the extracted root revealed evidence of deposition of hard tissue at the root apex despite the fact that there was overfilling. This tissue resembled the cementum of the root and appeared to be calcified. Furthermore, it seemed to be tightly attached to the surface of the cementum and it adapted closely to the overextended gutta-percha. The rough appearance of the rest of the root surface around the apex led to an assumption that, on this rough surface, more of this tissue may have been attached and had possibly been destroyed during the extraction of the root. Although a histological examination of this newly formed hard tissue was not performed, it is believed to be secondary cementum which was deposited in the areas of the root resorption. Possibly this deposition constituted an effort by the local defence mechanisms of the periapical tissues to isolate the foreign materials (gutta-percha and sealer). Finally, although in the postoperative radiograph the root canal filling in the apical third appears to be complete, in the SEM photographs a gap is evident between the newly formed tissue and the gutta-percha master cone. This gap was possibly created when the tooth was extracted or during specimen preparation for the SEM. In conclusion, although there was substantial extrusion of filling materials in the periapical area, long-term healing with secondary cementum deposition at the apex and resolution of lesion occurred and the case was considered to be successful. Obviously, these findings should not encourage dentists to overfill root canals, but they confirm the importance of chemomechanical preparation and complete obturation of the root canal, as well as the low toxicity of gutta-percha.
case_report.pdf


Σχόλια