



28/08/2018 0 Σχόλια
Radiographic quality of root fillings performed by undergraduate students
M. G. Khabbaz, E. Protogerou & E. Douka
Department of Endodontics, Faculty of Dentistry, University of Athens, Athens, Greece
Abstract
Khabbaz MG, Protogerou E, Douka E. Radiographic quality of root fillings performed by undergraduate students. International Endodontic Journal, 43, 499–508, 2010.
Aim
To evaluate the radiographic technical quality of root fillings and the incidence of iatrogenic errors in treatment provided by undergraduate students.
Methodology
Endodontic records and periapical radiographs of 759 root filled teeth were selected following exclusion of 25 (3.3%). A final total of 734 cases were used to assess the technical quality of root fillings in 1109 root canals performed by 4th and 5th undergraduate students. Two variables were examined: the length and the density of the fillings, categorized as acceptable and non-acceptable. The presence of ledges, root perforation, foramen perforation and fractured instruments were also investigated. Chi-square tests were used for statistical analysis.
Results
Acceptable root fillings were found in 55% of canals. More ‘acceptable’ root fillings occurred in maxillary compared to mandibular teeth (58 and 51% respectively) (P < 0.05) and in anterior compared with premolar (71 and 61%) and molar root canals (39% respectively) (P < 0.05). Insignificantly more (5.4%) acceptable root fillings were provided by 5th year students. Most of the underfillings and iatrogenic errors were detected in molars for both academic years (53 and 65% respectively). Ledges were noted in 55% of cases treated by both academic years and significantly more foramen perforations were detected in the 5th compared with the 4th year students (P < 0.05).
Conclusions
There is a need to improve the technical quality of root fillings performed by the undergraduate students, especially in molar teeth.
Keywords: dental education, radiographic evaluation, root canal treatment, root filling, iatrogenic errors, undergraduate students.
Introduction
The technical quality of root canal treatment and the coronal restoration have an important bearing on the periapical health of root-filled teeth (Ng et al. 2008).
The European Society of Endodontology has published Undergraduate Curriculum Guidelines for Endodontology to encourage the development of highquality undergraduate dental education and acceptable standards of care in clinical endodontics (European Society of Endodontology 1994, 2001). These guidelines state that the graduating student will be expected to demonstrate the ability to perform satisfactory nonsurgical root canal treatment on single and multirooted teeth. This must include cleaning, shaping and filling of the root canal system. The student is also expected to understand the iatrogenic errors that may occur during nonsurgical root canal treatment and how to avoid them. Yet, in ‘Profile and Competences for the European Dentist’ published in November 2004 by the Association for Dental Education in Europe and the DentEd III Thematic Network Project, it was declared that Dentists are expected to act for the achievement of the total health of their patients through oral health management without supervision. These skills should be taught during the clinical semesters of their studies, where they have to reach a level of performance requiring some degree of accuracy consistent with patient well-being (Association for Dental Education in Europe and the DentEd III Thematic Network Plasschaert et al. 2004). Despite the aforementioned statements, there is evidence that inadequate root canal treatment performed by dentists, in many countries, is not the exception but the rule (Table 1). Furthermore, iatrogenic complications or procedural errors during root canal treatment performed either by undergraduate students or dentists, such as ledges, canal transportation, instrument separation etc., may result in incomplete cleaning and shaping of the canals with a severe consequence on the outcome (Crump & Natkin 1970, Kapalas & Lambrianidis 2000, Lambrianidis 2001, Peters 2004, Eleftheriadis & Lambrianidis 2005).
At the Dentistry School of Athens, undergraduate students in Endodontics must complete a pre-clinical course, which includes both theoretical and practical training. This course is held during the 5th and 6th semester of the third year of the dental degree program, which lasts for 5 years overall. During the completion of this study (2004–2006), the course included 26 h of lectures and 39 h of laboratory practical training for the 5th semester and 26 h of lectures and 26 h of laboratory practical training for the 6th semester. The teacher to students ratio was 1/15 and neither Ni–Ti instruments nor apex locators were employed at that time. Success in one written examination was required in order to proceed to clinical training in the 7th –10th semester. During the 4th year (7th and 8th semesters), which represent the 1st clinical year in endodontics, students had to attend 26 h of clinical seminars in conjunction with their clinical practice on patients. During the 2nd clinical year (9th and 10th semesters), students worked in multidisciplinary clinics to fulfil the
clinical requirements that include Periodontology, Operative Dentistry, fixed and removable Prosthetic Dentistry and Endodontics.
One reason cited for the relatively poor technical standards of root canal treatment amongst general practitioners may be the limited endodontic teaching received at Dental Schools (Qualtrough et al. 1999, Barrieshi-Nusair et al. 2004). Subsequently, an investigation of the possible relationship between pre-clinical education in endodontics and the effectiveness of the clinical work provided by undergraduate students would be of great interest.
The aim of this study was to evaluate the results of pre-clinical educational approaches in Endodontics for undergraduate students in the Dental School of the University of Athens, Greece. This was undertaken by examining the radiographic quality of root fillings and the incidence of iatrogenic errors caused by the 4th and 5th year undergraduate students during their clinical practice.
Materials and methods
Endodontic records from 759 completed root canal treatments (RCT) performed by undergraduate students with the same pre-clinical training at the Dental School of the University of Athens, between 2004 and 2006, were randomly selected for examination. The inclusion criteria for this selection were:
1 All root canal treatments performed by 4th and 5th year undergraduate dental students on completely formed permanent teeth.
2 Teeth treated using at least three, long cone/ paralleling technique, radiographs (preoperative, working-length (intermediate) and postoperative) of good quality that showed the entire length of the root and the periapical area. Cases with unreadable radiographs were excluded.
Treatments were conducted by students according to the following protocol: After consideration of the medical and dental history of each patient, local anaesthesia was administered if needed. Afterwards, rubber dam isolation, access preparation and determination of the working length using K-files with an intermediate radiograph was performed. Each root canal was instrumented with the step back technique, using stainless steel hand instruments (K–files of 0.02 taper), whilst in some cases Gates-Glidden drills were used in the coronal third of the root canals in order to facilitate straight line access. Root canals were irrigated with 3% NaOCl, whilst in cases of narrow and calcified canals Rc-Prep paste (Premier Dental Products Comp. Norristown, Philadelphia, USA) was also used.
All root canals were filled during a second session with gutta-percha cones and cement (Roth root canal cement type 811 elite grade, Chicago, IL. USA) with the technique of cold lateral condensation. All gutta-percha cones and spreaders were of 2% taper.
Evaluation of the technical quality of root filling was based on the immediate postoperative radiograph. Two variables were examined, the length and the density of the root canal fillings. Iatrogenic errors included ledges, perforations (root and apical foramen) and fractured instruments were also recorded. The detection of these errors was based on the comparison of initial, intermediate and final radiographs.
Evaluation of the final root filling was performed through magnifying lenses on a diaphanascope by three independent investigators. All investigators examined all cases. In cases of interexaminer disagreement (52 root canals), examiners came to a consensus. Measurements were recorded using a transparent ruler of 0.5 mm accuracy. In cases of maxillary premolars and mandibular molars, exposed with alteration in horizontal angulation by the students, it was considered that they had been exposed with a mesial angulation. Consequently, this fact rendered it possible to differentiate the palatal from the buccal root canal in maxillary premolars and the mesiobuccal from the mesiolingual root canal in mandibular molars according to Clark’s rule (Georig & Neaverth 1987).
Evaluation criteria
The technical quality of the root fillings and the presence of iatrogenic errors found on radiographs were evaluated, classified and recorded; root canal was the unit of assessment.
The criteria for radiographic classification of the technical quality of root fillings were based on two variables; length and density. They were classified as acceptable and unacceptable as follows:
1 Acceptable: The filling material ends 0–2 mm short of the radiographic apex with no voids visible within the material or between material and the root canal walls.
2 Unacceptable:
A Under-filled: The filling material ends more than 2 mm from the radiographic apex.
B Density problem: The filling material ends 0–2 mm short from the radiographic apex with visible voids within or between the material and the root canal walls.
C Over-filled: Materials extruded beyond the apex.
The criteria for radiographic classification of the iatrogenic errors were based on:
1 Ledge: A ledge was considered present if the apical extent of gutta-percha in the final radiograph deviated from the original curvature compared with the working-length radiograph.
2 Perforation: A perforation was diagnosed when extrusion of materials was detected in any area of the root (lateral wall or the foramen of the root).
3 Fractured instrument: They were diagnosed through observation of the final radiograph and according to the radiopacity between the filling material and fractured instrument.
Statistical analysis
Data were expressed as frequencies and percentages. Differences in categorical variables were assessed using Pearson’s chi square test. Bonferroni–Holmes correction was applied in order to maintain a familywise a < 0.05, in cases of multiple comparisons. All tests were two sided. Differences were considered as statistically significant if the null hypothesis could be rejected with>95% confidence ( P < 0.05).
Results
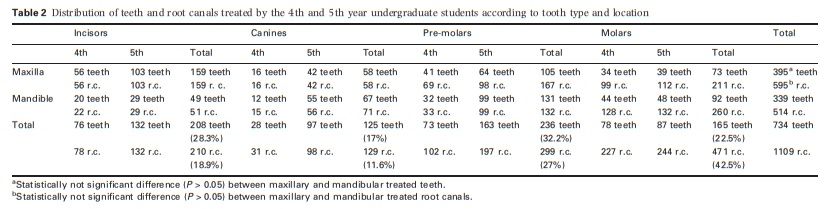
The total number of collected cases that received root canal treatment by the 4th and 5th year students was 759. From those 25 (3.3%) were excluded because of radiographic deficiencies such as over-exposure or over-development, under-fixing or abrasion, superimposition of root canals and anatomical noise from overlying structures. Finally, 734 teeth corresponding to 1109 root canals were included. The distribution of this sample according to the tooth type and location is detailed in Table 2. More maxillary teeth (395 teeth) and root canals (595 canals) were treated than mandibular teeth (339 teeth) and canals (514 canals). The difference was not significant ( P> 0.05). However, the distribution of frequencies of the various treated tooth types differed significantly between the arches (P < 0.001). In the maxilla, the most common tooth types were incisors and premolars. In the mandible, the pre-dominant types were premolars and molars. The frequencies of RCT amongst different tooth types differed significantly ( P < 0.001). Molars exhibited the highest number of completed RCT (42.5%), even though they were the third most commonly treated group of teeth. Specifically, 2.9 root canals on average
per tooth were treated in the molar group, a more than 200% increased frequency, compared to the other groups in both arches. From the same table, it can be noted that 4th and 5th year students performed 438 and 671 RCT on 255 and 479 teeth, respectively, which means that 5th year students operated on 88% more teeth and 53% more root canals than 4th year students.
Technical quality of root fillings
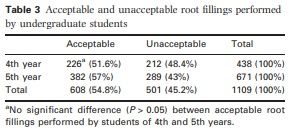
From 438 RCTs performed in the 4th year of study, acceptable fillings were detected in 226 (51.6%). From 671 RCTs performed in the 5th year of study, acceptable fillings were detected in 382 (57%) and in both academic years the percentage of acceptable fillings was (54.8%) (Table 3).
From the 1109 root canals treated by the students in both academic years, 595 were in the maxilla, from which 345 (58%) were acceptable. Of the 514 in the mandible, 263 (51.2%) were acceptable. Significantly more acceptable root fillings were detected in the maxilla than in the mandible (P < 0.05) (Table 4).
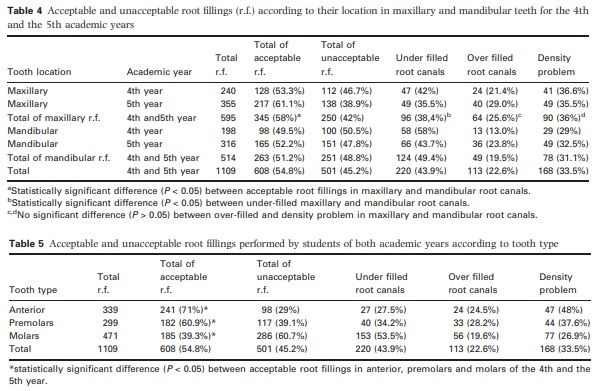
In both academic years, unacceptable root fillings were detected in 501 root canals, from which 250 were in the maxilla and 251 in the mandible. Even though the frequency of unacceptable root fillings was almost identical between maxilla and mandible (250 vs 251), the distribution of fault subgroups significantly differed between the two arches. Maxillary root canals exhibited a similar frequency of under-filling and canals with density problems (38.4% and 36%, respectively), which were the pre-dominant causes for unacceptable fillings. On the other hand, in mandibular canals, under-filling was by far the most common cause, responsible for 49.4% of unacceptable root fillings. Fillings with density problems only and over-fillings were detected respectively, in 90 (36%) and 64 (25.6%) root canals in the maxilla, in 78 (31.1%) and 49 (19.5%) respectively in the mandible with no significant differences between them (P> 0.05) (Table 4).
Of the 1109 root canals receiving treatment by the students of both academic years, 339 were anterior teeth, 299 pre-molars and 471 molars. Acceptable fillings were found respectively in 241 (71%), 182 (60.9%) and 185 (39.3%). Students of both years exhibited a significantly lower ratio of acceptable root fillings in molars, compared to anterior teeth (P < 0.05) and pre-molars (P < 0.05).
Thus, there was a statistically significant difference (P < 0.05) between acceptable root fillings performed in anterior, pre-molars and molars with descending tendency, with the best in anterior and the worst in molar teeth, for both academic years (Table 5). The total of unacceptable root fillings and the causes of the inadequacy are shown for 4th and 5th year students in Table 5.
Iatrogenic errors
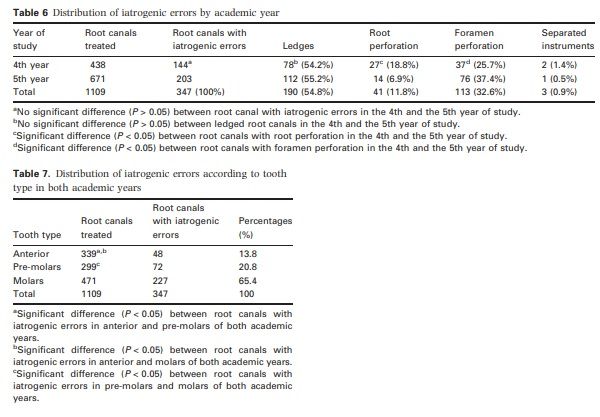
During their clinical training on patients, students of the 4th year created iatrogenic errors in 144 root canals out of 438 (32.9%) and of the 5th year in 203
out of 671 (30.3%). The difference was not significant (P> 0.05) (Table 6). The distribution of frequencies of different types of iatrogenic errors differed significantly between 4th and 5th year students (P < 0.01). Even though the percentages of ledges in root canals with iatrogenic errors were similar (P> 0.05), 5th year students created root perforations in only 14 root canals (6.9%), which was 63.1% fewer than the 4th year students (P < 0.05). However, they created foramen perforations in 76 root canals (37.4%), which was 40% higher than foramen perforations created by the 4th year students (37 root canals 25.7%) (P < 0.05) (Table 6).
Iatrogenic errors were detected in 347 root canals for both academic years from which 48 (13.8%) were in anterior teeth, 72 (20.8%) in pre-molars and 227 (65.4%) in molars. The frequency of iatrogenic errors differed significantly between tooth types (P < 0.001). Molars exhibited the highest frequency of iatrogenic errors and anterior teeth the lowest. All differences between frequencies amongst the various tooth types were statistically significant (P < 0.05) (Table 7).
Discussion
The material used in this study consisted of selected endodontic records and periapical radiographs of patients who received RCT. Only periapical radiographs were used and at least three preoperative, intermediate and postoperative were needed for each case to be included. In total 1109 RCT were considered in both jaws with no significant difference between the number of RCT performed in the maxilla or in the mandible. In this sample, it was found that students of both academic years treated more root canals in molars than in any other tooth group and, they conducted more RCT in 5th than in 4th year. In several studies, periapical health and improved outcome of RCT were most likely to be associated with dense root fillings, 0 to within 2 mm from the radiographic apex (Saunders et al. 1997, Chugal et al. 2003, Ng et al. 2008). These radiographic criteria were used in the present study to assess the quality of root fillings performed by undergraduate students. Similar criteria were used by others (Buckley & Spangberg 1995, Boltacz-Rzepkowska & Pawlicka 2003, Barrieshi-Nusair et al. 2004).
The evaluation of the radiographic technical quality of root fillings in anterior and posterior teeth, performed by 4th and 5th year dental students, revealed that overall 54.8% were technically acceptable. Whilst it is difficult to compare this finding with other educational institutes, the trend appears similar to some (Eleftheriadis & Lambrianidis 2005) and at variance to others (Hayes et al. 2001, Barrieshi-Nusair et al. 2004, Lynch & Burke 2006, Er et al. 2006, Moussa-Badran et al. 2008). These differences may occur because of different criteria used in evaluation, materials, educational system, methods etc. For example, in the study of Lynch & Burke (2006) 63 root fillings out of 100 (63%) performed on single-rooted teeth were acceptable. In this study, the evaluation of the radiographic technical quality of the root fillings was performed on a small number of teeth with one straight root canal. Although the ratio in the present study on anterior teeth only was higher (71%), this figure does not reflect the real situation of the clinical skill of the undergraduate students, because they also have to complete endodontic therapy and show their skill on multi-rooted teeth (European Society of Endodontology 1994, 2001).
Comparing the present results with others (see Table 1), it seems that the mean percentage of adequate fillings performed by undergraduate students (54.8%) was relatively high. However, under-reporting of problems may have occurred because of the twodimensional radiographic images and the unknown number of cases referred to the post-graduate clinic as a result of difficulties or because of technically impairment by the under-graduate students.
Different surveys have demonstrated that general practitioners, even the recently qualified, do not follow guidelines taught during their basic education (Helminen et al. 2000, Stewardson 2001, 2002, Hill & Rubel 2008). Thus, it can be speculated that the percentage of 54.8% will probably be decreased amongst graduates. Undoubtedly, this needs to be improved. However, it is already known from an investigation of the frequency and distribution of root-filled teeth and apical periodontitis in a Greek population that the prevalence of apical periodontitis associated with the root-filled teeth was 60% (Georgopoulou et al. 2005). It is well established that the presence of apical periodontitis in root-filled teeth is often associated with inadequate root fillings.
For both academic years, the highest percentage of acceptable root fillings was noted in anterior teeth and the lowest in posterior teeth, especially molars. Similar results were found in other educational institutes (Barrieshi-Nusair et al. 2004, Eleftheriadis & Lambrianidis 2005). Furthermore, in several studies concerning national populations, it was detected that molar teeth had significantly higher levels of apical periodontitis compared with other teeth (Kirkevang et al. 2001, Jimenez-Pinzon et al. 2004, Georgopoulou et al. 2005, Loftus et al. 2005, Ridell et al. 2006). Thus, it is apparent that in Dental Schools and dental practice, it is difficult to treat molar teeth successfully. Accordingly, modification of the educational program needs to take place to emphasize the differences between treating molars versus anterior teeth and to acquire the clinical skill requested. Specifically, the introduction of hand and rotary Ni–Ti instruments for the instrumentation of molar root canals may be of benefit. Clinical research has demonstrated that there was a higher incidence of procedural errors and a lower success rate for primary RCT of molar teeth prepared with stainless steel files compared with the use of Ni–Ti instruments in a continuous reaming action (Cheung & Liu 2009).
The percentage of unacceptable root fillings was 45.2%. The reason for this high percentage is probably correlated to inadequate chemomechanical preparation or/and the filling of the root canals. The technique taught for chemomechanical preparation was traditional serial step-back with stainless steel K-files used in a filing motion and for the filling of root canals was lateral condensation of cold gutta-percha. It is known that the step-back technique used by inexperienced students may produce procedural errors such as ledges, blocking and transportation of the root canal, which may lead to incomplete cleaning and underfilling (Greene & Krell 1990, Gambarini 1999, Kfir et al. 2004). Moreover, the usage of stainless steel instruments may produce a high incidence of procedural errors, which may reduce the prognosis (Cheung & Liu 2009).
Furthermore, the lateral condensation of cold guttapercha in a nonflared or minimally flared root canal may create voids. Following this study, it was decided to emphasize on using Ni–Ti instruments and preflaring of the root canal before the measurement of the working length and to recapitulate between instruments with a small file to loosen the accumulated debris in the apical portion of the root canal.
One of the aims of academic teachers must be to improve knowledge and skills through the improvement of the educational program. The educational level offered in Endodontics has been a topic of great interest (Qualtrough & Dummer 1997, Qualtrough et al. 1999, Hayes et al. 2001, Petersson et al. 2002, BarrieshiNusair et al. 2004, Eleftheriadis & Lambrianidis 2005, Lynch & Burke 2006, Er et al. 2006, Sonntag et al. 2008). The quality of education is a resultant of many factors such as time devoted to theoretical and practical teaching and training (pre-clinical and clinical), the ratio of supervisors: students, the clinical and scientific level of teachers if they are specialized or not, the teaching aids, the assessment methods, etc.
Aiming to enhance the clinical performance of undergraduate students in endodontics, changes have already been made to the pre-clinical course. These include better theoretical teaching and laboratory exercises and better training of teachers because of special staff-seminars organized by the administration of our School. These changes have led to the following:
1 Increase in laboratory training time,
2 Improvement of the teacher to student ratio from 1/ 15 to 1/6,
3 Involvement of specialist endodontists and third year postgraduate students in pre-clinical education,
4 Insertion of flexible laboratory seminars that are supported by practical demonstrations of each exercise immediately before training,
5 Implementation of audiovisual technology in education,
6 Use of new technology such as the rotary instrumentation and the electronic measurement of working length,
7 Addition of seminars on molar endodontics and increasing the number of molars treated in the laboratory,
8 Application of an assessment system that includes student self-assessment and staff assessment, theoretical and practical examination on an extracted tooth at the end of the 5th and the 6th semester
9 Adoption of flexible examinations that consist of the summation of three written test with the mean average degree of the theoretical and practical assessment in the laboratory.
Finally, it will be of great interest to repeat the same research in the future to assure the predictability of the new educational measures.
Conclusions
The radiographic quality of RCT performed by the 4th and the 5th year undergraduate students in the School of Dentistry of the University of Athens was acceptable in 54.8% of cases. As a result, there is a need to improve the quality of the RCTs performed by undergraduate students, through the revision of the preclinical educational program in Endodontics. Special emphasis must be placed on the educational methods and training of students providing root filling on molar teeth.
Acknowledgements
The authors thank Dr Stefaniotis Theodoros for his assistance in the statistical analysis of this study.
References
Association for Dental Education in Europe and the DentEd III Thematic Network. Plasschaert AJM, Holbrook WP, Delap E, Martinez C, Walmsley AD (2004) Profile and Competences for the European Dentist. (http://www.adee.dental.tcd.ie/).
Barrieshi-Nusair KM, Al-Omari MA, Al-Hiyasat AS (2004) Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Center in Jordan. Journal of Dentistry 32, 301–7.
Bierenkrant DE, Parashos P, Messer HH (2008) The technical quality of nonsurgical root canal treatment performed by a selected cohort of Australian endodontists. International Endodontic Journal 41, 561–70.
Boltacz-RzepkowskaE,PawlickaH (2003)Radiographicfeatures and outcome of root canal treatment carried out in the Lodz region of Poland. International Endodontic Journal 36, 27–32.
Boucher Y, Matossian L, Rilliard F, Machtou P (2002) Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. International Endodontic Journal 35, 229–38.
Buckley M, Spangberg LSW (1995) The prevalence and technical quality of endodontic treatment in an American subpopulation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 79, 92–100.
Chen CY, Hasselgren G, Serman N, Elkind MS, Desvarieux M, Engebretson SP (2007) Prevalence and quality of endodontic treatment in the Northern Manhattan elderly. Journal of Endodontics 33, 230–4.
Cheung GS, Liu CS (2009) A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. Journal of Endodontics 35, 938–43.
Chueh LH, Chen SC, Lee CM et al. (2003) Technical quality of root canal treatment in Taiwan. International Endodontic Journal 36, 416–22. Chugal NM, Clive JM, Spangberg LSW (2003) Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 96, 81–90.
Crump MC, Natkin E (1970) Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. Journal of American Denal Association 80, 1341–7.
De Moor RJ, Hommez GM, De Boever JG, Delme KI, Martens GE (2000) Periapical health related to the quality of root canal treatment in a Belgian population. International Endodontic Journal 33, 113–20.
Eleftheriadis G, Lambrianidis T (2005) Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. International Endodontic Journal 38, 725–34.
Er O, Sagsen B, Maden M, Cinar S, Kahraman Y (2006) Radiographic technical quality of root fillings performed by dental students in Turkey. International Endodontic Journal 39, 867–72.
European Society of Endodontology (1994) Consensus report of the European Society of Endodontology on quality guidelines for endodontic treatment. International Endodontic Journal 27, 115–24.
European Society of Endodontology (2001) Undergraduate curriculum guidelines for Endodontology. International Endodontic Journal 34, 574–80.
Gambarini G (1999) Shaping and cleaning the root canal system. A scaning electron microscopic evaluation of a new instrumentation and irrigation technique. Journal of Endodontics 25, 800–3.
Georgopoulou M, Spanaki-Voreadi A, Pantazis N, Kontakiotis E (2005) Frequency and distribution of root filled teeth and apical periodontitis in a Greek population. International Endodontic Journal 38, 105–11.
Georig A, Neaverth E (1987) A simplified look at the buccal object rule in endodontics. Journal of Endodontics 13, 570–2.
Greene KJ, Krell KV (1990) Clinical factors associated with ledged canals in maxillary and mandibular molars. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 70, 490–7.
Hayes SJ, Gibson M, Hammond M, Bryant ST, Dummer PMH (2001) An audit of root canal treatment performed by undergraduate students. International Endodontic Journal 34, 501–5.
Helminen SE, Vehkalahti M, Kerosuo E, Murtomaa H (2000) Quality evaluation of process of root canal treatments performed on young adults in Finnish public oral health service. Journal of Dentistry 28, 227–32.
Hill EE, Rubel BS (2008) Do dental educators need to improve their approach to teaching rubber dam use? Journal of Dental Education 72, 1177–81.
Jimenez-Pinzon A, Segura-Egea JJ, Poyato-Ferrera M, VelascoOrtega E, Rıos-Santos JV (2004) Prevalence of apical periodontitis and frequency of root filled teeth in an adult Spanish population. International Endodontic Journal 37, 167–73.
Kapalas A, Lambrianidis T (2000) Factors associated with root canal ledging during nstrumentation. Endodontics and Dental Traumatology 16, 229–31.
Kfir A, Rosenberg E, Zuckerman O, Tamse A, Fuss Z (2004) Comparison of procedural errors resulting during root canal preparations completed by senior dental students in patients using an ‘8-step method’ versus ‘serial step-back technique’. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 97, 745–8.
Kirkevang LL, Horsted-Bindslev P, Ørstavik D, Wenzel A (2001) A comparison of the quality of root canal treatment in two Danish subpopulations examined 1974-75 and 1997-98. International Endodontic Journal 34, 607–12.
Lambrianidis T (2001) Risk Management in root canal treatment, 1st edn. Thessaloniki: University Studio Press. Loftus JJ, keating AP, McCartan BE (2005) Periapical status and quality of endodontic treatment in an adult Irish population. International Endodontic Journal 38, 81–6.
Lynch CD, Burke FM (2006) Quality of root canal fillings performed by undergraduate dental students on singlerooted teeth. European Journal of Dental Education 10, 67–72.
Moussa-Badran S, Roy B, Bessart du Parc AS, Bruyant M, Lefevre B, Maurin JC (2008) Technical quality of root fillings performed by dental students at the dental teaching centre in Reims, France. International Endodontic Journal 41, 679– 84.
Ng Y-L, Mann V, Rahbaran S, Lewsey J, Gulabivala K (2008) Outcome of primary root canal treatment: systematic review of the literature – Part 2 Influence of clinical factors. International Endodontic Journal 41, 6–31.
Peters OA (2004) Current challenges and concepts in the preparation of root canal systems: a review. Journal of Endodontics 30, 559–67.
Petersson K, Olsson H, So¨derstro¨m C, Fouilloux I, Jegat N, Le´vy G (2002) Undergraduate education in endodontology at two European dental schools. A comparison between the Faculty of Odontology, Malmo¨ University, Malmo¨, Sweden and Faculty of Odontology, Paris 5 University (Rene´ Descartes), France. European Journal of Dental Education 6, 176–81.
Qualtrough AJE, Dummer PMH (1997) Undergraduate endodontic teaching in the United Kngdom: an update. International Endodontic Journal 30, 234–40.
Qualtrough A, Whitworth J, Dummer P (1999) Preclinical endodontology: an international comparison. International Endodontic Journal 32, 406–14.
Ridell K, Petersson A, Matsson L, Mejare I (2006) Periapical status and technical quality of root filled teeth in Swedish adolescents and young adults: a retrospective study. Acta Odontontologica Scandinavia 64, 104–10.
Saunders WP, Saunders EM, Sadiq J, Cruickshank E (1997) Technical standard of root canal treatment in an adult Scottish sub-population. British Dental Journal 182, 382–6.
Segura-Egea JJ, Jime nez-Pinzo A, Poyato-Ferrera M, VelascoOrtega E, Rıos-Santos JV (2004) Periapical status and quality of root fillings and coronal restorations in an adult Spanish population. International Endodontic Journal 37, 525–30.
Siqueira JF Jr, Roˆc¸as IN, Alves FR, Campos LC (2005) Periradicular status related to the quality of coronal restorations and root canal fillings in a Brazilian population. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 100, 369–74.
Sonntag D, Barwald R, Hulsmann M, Stachniss V (2008) Preclinical endodontics: a survey amongst German dental schools. International Endodontic Journal 41, 863–8.
Stewardson DA (2001) Endodontic standards in general dental practice–a survey in Birmingham, Part I. The European Journal of Prosthodontics and Restorative Dentistry 9, 107–12.
Stewardson DA (2002) Endodontics and new graduates: part I, Practice vs training. The European Journal of Prosthodontics and Restorative Dentistry 10, 131–7.
Sunay H, Tanalp J, Dikbas I, Bayirli G (2007) Cross-sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. International Endodontic Journal 40, 139–45.
Toure´ B, Kane AW, Sarr M, Ngom CT, Boucher Y (2008) Prevalence and technical quality of root fillings in Dakar, Senegal. International Endodontic Journal 41, 41–9.
Weiger R, Hitzler S, Hermle G, Lost C (1997) Periapical status, quality of root canal fillings and estimated endodontic treatment needs in an urban German population. Endodontics and Dental Traumatology 13, 69–74.
Radiographic_quality_of_root_fillings.pdf
Department of Endodontics, Faculty of Dentistry, University of Athens, Athens, Greece
Abstract
Khabbaz MG, Protogerou E, Douka E. Radiographic quality of root fillings performed by undergraduate students. International Endodontic Journal, 43, 499–508, 2010.
Aim
To evaluate the radiographic technical quality of root fillings and the incidence of iatrogenic errors in treatment provided by undergraduate students.
Methodology
Endodontic records and periapical radiographs of 759 root filled teeth were selected following exclusion of 25 (3.3%). A final total of 734 cases were used to assess the technical quality of root fillings in 1109 root canals performed by 4th and 5th undergraduate students. Two variables were examined: the length and the density of the fillings, categorized as acceptable and non-acceptable. The presence of ledges, root perforation, foramen perforation and fractured instruments were also investigated. Chi-square tests were used for statistical analysis.
Results
Acceptable root fillings were found in 55% of canals. More ‘acceptable’ root fillings occurred in maxillary compared to mandibular teeth (58 and 51% respectively) (P < 0.05) and in anterior compared with premolar (71 and 61%) and molar root canals (39% respectively) (P < 0.05). Insignificantly more (5.4%) acceptable root fillings were provided by 5th year students. Most of the underfillings and iatrogenic errors were detected in molars for both academic years (53 and 65% respectively). Ledges were noted in 55% of cases treated by both academic years and significantly more foramen perforations were detected in the 5th compared with the 4th year students (P < 0.05).
Conclusions
There is a need to improve the technical quality of root fillings performed by the undergraduate students, especially in molar teeth.
Keywords: dental education, radiographic evaluation, root canal treatment, root filling, iatrogenic errors, undergraduate students.
Introduction
The technical quality of root canal treatment and the coronal restoration have an important bearing on the periapical health of root-filled teeth (Ng et al. 2008).
The European Society of Endodontology has published Undergraduate Curriculum Guidelines for Endodontology to encourage the development of highquality undergraduate dental education and acceptable standards of care in clinical endodontics (European Society of Endodontology 1994, 2001). These guidelines state that the graduating student will be expected to demonstrate the ability to perform satisfactory nonsurgical root canal treatment on single and multirooted teeth. This must include cleaning, shaping and filling of the root canal system. The student is also expected to understand the iatrogenic errors that may occur during nonsurgical root canal treatment and how to avoid them. Yet, in ‘Profile and Competences for the European Dentist’ published in November 2004 by the Association for Dental Education in Europe and the DentEd III Thematic Network Project, it was declared that Dentists are expected to act for the achievement of the total health of their patients through oral health management without supervision. These skills should be taught during the clinical semesters of their studies, where they have to reach a level of performance requiring some degree of accuracy consistent with patient well-being (Association for Dental Education in Europe and the DentEd III Thematic Network Plasschaert et al. 2004). Despite the aforementioned statements, there is evidence that inadequate root canal treatment performed by dentists, in many countries, is not the exception but the rule (Table 1). Furthermore, iatrogenic complications or procedural errors during root canal treatment performed either by undergraduate students or dentists, such as ledges, canal transportation, instrument separation etc., may result in incomplete cleaning and shaping of the canals with a severe consequence on the outcome (Crump & Natkin 1970, Kapalas & Lambrianidis 2000, Lambrianidis 2001, Peters 2004, Eleftheriadis & Lambrianidis 2005).
At the Dentistry School of Athens, undergraduate students in Endodontics must complete a pre-clinical course, which includes both theoretical and practical training. This course is held during the 5th and 6th semester of the third year of the dental degree program, which lasts for 5 years overall. During the completion of this study (2004–2006), the course included 26 h of lectures and 39 h of laboratory practical training for the 5th semester and 26 h of lectures and 26 h of laboratory practical training for the 6th semester. The teacher to students ratio was 1/15 and neither Ni–Ti instruments nor apex locators were employed at that time. Success in one written examination was required in order to proceed to clinical training in the 7th –10th semester. During the 4th year (7th and 8th semesters), which represent the 1st clinical year in endodontics, students had to attend 26 h of clinical seminars in conjunction with their clinical practice on patients. During the 2nd clinical year (9th and 10th semesters), students worked in multidisciplinary clinics to fulfil the
clinical requirements that include Periodontology, Operative Dentistry, fixed and removable Prosthetic Dentistry and Endodontics.
One reason cited for the relatively poor technical standards of root canal treatment amongst general practitioners may be the limited endodontic teaching received at Dental Schools (Qualtrough et al. 1999, Barrieshi-Nusair et al. 2004). Subsequently, an investigation of the possible relationship between pre-clinical education in endodontics and the effectiveness of the clinical work provided by undergraduate students would be of great interest.
The aim of this study was to evaluate the results of pre-clinical educational approaches in Endodontics for undergraduate students in the Dental School of the University of Athens, Greece. This was undertaken by examining the radiographic quality of root fillings and the incidence of iatrogenic errors caused by the 4th and 5th year undergraduate students during their clinical practice.
Materials and methods
Endodontic records from 759 completed root canal treatments (RCT) performed by undergraduate students with the same pre-clinical training at the Dental School of the University of Athens, between 2004 and 2006, were randomly selected for examination. The inclusion criteria for this selection were:
1 All root canal treatments performed by 4th and 5th year undergraduate dental students on completely formed permanent teeth.
2 Teeth treated using at least three, long cone/ paralleling technique, radiographs (preoperative, working-length (intermediate) and postoperative) of good quality that showed the entire length of the root and the periapical area. Cases with unreadable radiographs were excluded.
Treatments were conducted by students according to the following protocol: After consideration of the medical and dental history of each patient, local anaesthesia was administered if needed. Afterwards, rubber dam isolation, access preparation and determination of the working length using K-files with an intermediate radiograph was performed. Each root canal was instrumented with the step back technique, using stainless steel hand instruments (K–files of 0.02 taper), whilst in some cases Gates-Glidden drills were used in the coronal third of the root canals in order to facilitate straight line access. Root canals were irrigated with 3% NaOCl, whilst in cases of narrow and calcified canals Rc-Prep paste (Premier Dental Products Comp. Norristown, Philadelphia, USA) was also used.
All root canals were filled during a second session with gutta-percha cones and cement (Roth root canal cement type 811 elite grade, Chicago, IL. USA) with the technique of cold lateral condensation. All gutta-percha cones and spreaders were of 2% taper.
Evaluation of the technical quality of root filling was based on the immediate postoperative radiograph. Two variables were examined, the length and the density of the root canal fillings. Iatrogenic errors included ledges, perforations (root and apical foramen) and fractured instruments were also recorded. The detection of these errors was based on the comparison of initial, intermediate and final radiographs.
Evaluation of the final root filling was performed through magnifying lenses on a diaphanascope by three independent investigators. All investigators examined all cases. In cases of interexaminer disagreement (52 root canals), examiners came to a consensus. Measurements were recorded using a transparent ruler of 0.5 mm accuracy. In cases of maxillary premolars and mandibular molars, exposed with alteration in horizontal angulation by the students, it was considered that they had been exposed with a mesial angulation. Consequently, this fact rendered it possible to differentiate the palatal from the buccal root canal in maxillary premolars and the mesiobuccal from the mesiolingual root canal in mandibular molars according to Clark’s rule (Georig & Neaverth 1987).
Evaluation criteria
The technical quality of the root fillings and the presence of iatrogenic errors found on radiographs were evaluated, classified and recorded; root canal was the unit of assessment.
The criteria for radiographic classification of the technical quality of root fillings were based on two variables; length and density. They were classified as acceptable and unacceptable as follows:
1 Acceptable: The filling material ends 0–2 mm short of the radiographic apex with no voids visible within the material or between material and the root canal walls.
2 Unacceptable:
A Under-filled: The filling material ends more than 2 mm from the radiographic apex.
B Density problem: The filling material ends 0–2 mm short from the radiographic apex with visible voids within or between the material and the root canal walls.
C Over-filled: Materials extruded beyond the apex.
The criteria for radiographic classification of the iatrogenic errors were based on:
1 Ledge: A ledge was considered present if the apical extent of gutta-percha in the final radiograph deviated from the original curvature compared with the working-length radiograph.
2 Perforation: A perforation was diagnosed when extrusion of materials was detected in any area of the root (lateral wall or the foramen of the root).
3 Fractured instrument: They were diagnosed through observation of the final radiograph and according to the radiopacity between the filling material and fractured instrument.
Statistical analysis
Data were expressed as frequencies and percentages. Differences in categorical variables were assessed using Pearson’s chi square test. Bonferroni–Holmes correction was applied in order to maintain a familywise a < 0.05, in cases of multiple comparisons. All tests were two sided. Differences were considered as statistically significant if the null hypothesis could be rejected with>95% confidence ( P < 0.05).
Results
The total number of collected cases that received root canal treatment by the 4th and 5th year students was 759. From those 25 (3.3%) were excluded because of radiographic deficiencies such as over-exposure or over-development, under-fixing or abrasion, superimposition of root canals and anatomical noise from overlying structures. Finally, 734 teeth corresponding to 1109 root canals were included. The distribution of this sample according to the tooth type and location is detailed in Table 2. More maxillary teeth (395 teeth) and root canals (595 canals) were treated than mandibular teeth (339 teeth) and canals (514 canals). The difference was not significant ( P> 0.05). However, the distribution of frequencies of the various treated tooth types differed significantly between the arches (P < 0.001). In the maxilla, the most common tooth types were incisors and premolars. In the mandible, the pre-dominant types were premolars and molars. The frequencies of RCT amongst different tooth types differed significantly ( P < 0.001). Molars exhibited the highest number of completed RCT (42.5%), even though they were the third most commonly treated group of teeth. Specifically, 2.9 root canals on average
per tooth were treated in the molar group, a more than 200% increased frequency, compared to the other groups in both arches. From the same table, it can be noted that 4th and 5th year students performed 438 and 671 RCT on 255 and 479 teeth, respectively, which means that 5th year students operated on 88% more teeth and 53% more root canals than 4th year students.
Technical quality of root fillings
From 438 RCTs performed in the 4th year of study, acceptable fillings were detected in 226 (51.6%). From 671 RCTs performed in the 5th year of study, acceptable fillings were detected in 382 (57%) and in both academic years the percentage of acceptable fillings was (54.8%) (Table 3).
From the 1109 root canals treated by the students in both academic years, 595 were in the maxilla, from which 345 (58%) were acceptable. Of the 514 in the mandible, 263 (51.2%) were acceptable. Significantly more acceptable root fillings were detected in the maxilla than in the mandible (P < 0.05) (Table 4).
In both academic years, unacceptable root fillings were detected in 501 root canals, from which 250 were in the maxilla and 251 in the mandible. Even though the frequency of unacceptable root fillings was almost identical between maxilla and mandible (250 vs 251), the distribution of fault subgroups significantly differed between the two arches. Maxillary root canals exhibited a similar frequency of under-filling and canals with density problems (38.4% and 36%, respectively), which were the pre-dominant causes for unacceptable fillings. On the other hand, in mandibular canals, under-filling was by far the most common cause, responsible for 49.4% of unacceptable root fillings. Fillings with density problems only and over-fillings were detected respectively, in 90 (36%) and 64 (25.6%) root canals in the maxilla, in 78 (31.1%) and 49 (19.5%) respectively in the mandible with no significant differences between them (P> 0.05) (Table 4).
Of the 1109 root canals receiving treatment by the students of both academic years, 339 were anterior teeth, 299 pre-molars and 471 molars. Acceptable fillings were found respectively in 241 (71%), 182 (60.9%) and 185 (39.3%). Students of both years exhibited a significantly lower ratio of acceptable root fillings in molars, compared to anterior teeth (P < 0.05) and pre-molars (P < 0.05).
Thus, there was a statistically significant difference (P < 0.05) between acceptable root fillings performed in anterior, pre-molars and molars with descending tendency, with the best in anterior and the worst in molar teeth, for both academic years (Table 5). The total of unacceptable root fillings and the causes of the inadequacy are shown for 4th and 5th year students in Table 5.
Iatrogenic errors
During their clinical training on patients, students of the 4th year created iatrogenic errors in 144 root canals out of 438 (32.9%) and of the 5th year in 203
out of 671 (30.3%). The difference was not significant (P> 0.05) (Table 6). The distribution of frequencies of different types of iatrogenic errors differed significantly between 4th and 5th year students (P < 0.01). Even though the percentages of ledges in root canals with iatrogenic errors were similar (P> 0.05), 5th year students created root perforations in only 14 root canals (6.9%), which was 63.1% fewer than the 4th year students (P < 0.05). However, they created foramen perforations in 76 root canals (37.4%), which was 40% higher than foramen perforations created by the 4th year students (37 root canals 25.7%) (P < 0.05) (Table 6).
Iatrogenic errors were detected in 347 root canals for both academic years from which 48 (13.8%) were in anterior teeth, 72 (20.8%) in pre-molars and 227 (65.4%) in molars. The frequency of iatrogenic errors differed significantly between tooth types (P < 0.001). Molars exhibited the highest frequency of iatrogenic errors and anterior teeth the lowest. All differences between frequencies amongst the various tooth types were statistically significant (P < 0.05) (Table 7).
Discussion
The material used in this study consisted of selected endodontic records and periapical radiographs of patients who received RCT. Only periapical radiographs were used and at least three preoperative, intermediate and postoperative were needed for each case to be included. In total 1109 RCT were considered in both jaws with no significant difference between the number of RCT performed in the maxilla or in the mandible. In this sample, it was found that students of both academic years treated more root canals in molars than in any other tooth group and, they conducted more RCT in 5th than in 4th year. In several studies, periapical health and improved outcome of RCT were most likely to be associated with dense root fillings, 0 to within 2 mm from the radiographic apex (Saunders et al. 1997, Chugal et al. 2003, Ng et al. 2008). These radiographic criteria were used in the present study to assess the quality of root fillings performed by undergraduate students. Similar criteria were used by others (Buckley & Spangberg 1995, Boltacz-Rzepkowska & Pawlicka 2003, Barrieshi-Nusair et al. 2004).
The evaluation of the radiographic technical quality of root fillings in anterior and posterior teeth, performed by 4th and 5th year dental students, revealed that overall 54.8% were technically acceptable. Whilst it is difficult to compare this finding with other educational institutes, the trend appears similar to some (Eleftheriadis & Lambrianidis 2005) and at variance to others (Hayes et al. 2001, Barrieshi-Nusair et al. 2004, Lynch & Burke 2006, Er et al. 2006, Moussa-Badran et al. 2008). These differences may occur because of different criteria used in evaluation, materials, educational system, methods etc. For example, in the study of Lynch & Burke (2006) 63 root fillings out of 100 (63%) performed on single-rooted teeth were acceptable. In this study, the evaluation of the radiographic technical quality of the root fillings was performed on a small number of teeth with one straight root canal. Although the ratio in the present study on anterior teeth only was higher (71%), this figure does not reflect the real situation of the clinical skill of the undergraduate students, because they also have to complete endodontic therapy and show their skill on multi-rooted teeth (European Society of Endodontology 1994, 2001).
Comparing the present results with others (see Table 1), it seems that the mean percentage of adequate fillings performed by undergraduate students (54.8%) was relatively high. However, under-reporting of problems may have occurred because of the twodimensional radiographic images and the unknown number of cases referred to the post-graduate clinic as a result of difficulties or because of technically impairment by the under-graduate students.
Different surveys have demonstrated that general practitioners, even the recently qualified, do not follow guidelines taught during their basic education (Helminen et al. 2000, Stewardson 2001, 2002, Hill & Rubel 2008). Thus, it can be speculated that the percentage of 54.8% will probably be decreased amongst graduates. Undoubtedly, this needs to be improved. However, it is already known from an investigation of the frequency and distribution of root-filled teeth and apical periodontitis in a Greek population that the prevalence of apical periodontitis associated with the root-filled teeth was 60% (Georgopoulou et al. 2005). It is well established that the presence of apical periodontitis in root-filled teeth is often associated with inadequate root fillings.
For both academic years, the highest percentage of acceptable root fillings was noted in anterior teeth and the lowest in posterior teeth, especially molars. Similar results were found in other educational institutes (Barrieshi-Nusair et al. 2004, Eleftheriadis & Lambrianidis 2005). Furthermore, in several studies concerning national populations, it was detected that molar teeth had significantly higher levels of apical periodontitis compared with other teeth (Kirkevang et al. 2001, Jimenez-Pinzon et al. 2004, Georgopoulou et al. 2005, Loftus et al. 2005, Ridell et al. 2006). Thus, it is apparent that in Dental Schools and dental practice, it is difficult to treat molar teeth successfully. Accordingly, modification of the educational program needs to take place to emphasize the differences between treating molars versus anterior teeth and to acquire the clinical skill requested. Specifically, the introduction of hand and rotary Ni–Ti instruments for the instrumentation of molar root canals may be of benefit. Clinical research has demonstrated that there was a higher incidence of procedural errors and a lower success rate for primary RCT of molar teeth prepared with stainless steel files compared with the use of Ni–Ti instruments in a continuous reaming action (Cheung & Liu 2009).
The percentage of unacceptable root fillings was 45.2%. The reason for this high percentage is probably correlated to inadequate chemomechanical preparation or/and the filling of the root canals. The technique taught for chemomechanical preparation was traditional serial step-back with stainless steel K-files used in a filing motion and for the filling of root canals was lateral condensation of cold gutta-percha. It is known that the step-back technique used by inexperienced students may produce procedural errors such as ledges, blocking and transportation of the root canal, which may lead to incomplete cleaning and underfilling (Greene & Krell 1990, Gambarini 1999, Kfir et al. 2004). Moreover, the usage of stainless steel instruments may produce a high incidence of procedural errors, which may reduce the prognosis (Cheung & Liu 2009).
Furthermore, the lateral condensation of cold guttapercha in a nonflared or minimally flared root canal may create voids. Following this study, it was decided to emphasize on using Ni–Ti instruments and preflaring of the root canal before the measurement of the working length and to recapitulate between instruments with a small file to loosen the accumulated debris in the apical portion of the root canal.
One of the aims of academic teachers must be to improve knowledge and skills through the improvement of the educational program. The educational level offered in Endodontics has been a topic of great interest (Qualtrough & Dummer 1997, Qualtrough et al. 1999, Hayes et al. 2001, Petersson et al. 2002, BarrieshiNusair et al. 2004, Eleftheriadis & Lambrianidis 2005, Lynch & Burke 2006, Er et al. 2006, Sonntag et al. 2008). The quality of education is a resultant of many factors such as time devoted to theoretical and practical teaching and training (pre-clinical and clinical), the ratio of supervisors: students, the clinical and scientific level of teachers if they are specialized or not, the teaching aids, the assessment methods, etc.
Aiming to enhance the clinical performance of undergraduate students in endodontics, changes have already been made to the pre-clinical course. These include better theoretical teaching and laboratory exercises and better training of teachers because of special staff-seminars organized by the administration of our School. These changes have led to the following:
1 Increase in laboratory training time,
2 Improvement of the teacher to student ratio from 1/ 15 to 1/6,
3 Involvement of specialist endodontists and third year postgraduate students in pre-clinical education,
4 Insertion of flexible laboratory seminars that are supported by practical demonstrations of each exercise immediately before training,
5 Implementation of audiovisual technology in education,
6 Use of new technology such as the rotary instrumentation and the electronic measurement of working length,
7 Addition of seminars on molar endodontics and increasing the number of molars treated in the laboratory,
8 Application of an assessment system that includes student self-assessment and staff assessment, theoretical and practical examination on an extracted tooth at the end of the 5th and the 6th semester
9 Adoption of flexible examinations that consist of the summation of three written test with the mean average degree of the theoretical and practical assessment in the laboratory.
Finally, it will be of great interest to repeat the same research in the future to assure the predictability of the new educational measures.
Conclusions
The radiographic quality of RCT performed by the 4th and the 5th year undergraduate students in the School of Dentistry of the University of Athens was acceptable in 54.8% of cases. As a result, there is a need to improve the quality of the RCTs performed by undergraduate students, through the revision of the preclinical educational program in Endodontics. Special emphasis must be placed on the educational methods and training of students providing root filling on molar teeth.
Acknowledgements
The authors thank Dr Stefaniotis Theodoros for his assistance in the statistical analysis of this study.
References
Association for Dental Education in Europe and the DentEd III Thematic Network. Plasschaert AJM, Holbrook WP, Delap E, Martinez C, Walmsley AD (2004) Profile and Competences for the European Dentist. (http://www.adee.dental.tcd.ie/).
Barrieshi-Nusair KM, Al-Omari MA, Al-Hiyasat AS (2004) Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Center in Jordan. Journal of Dentistry 32, 301–7.
Bierenkrant DE, Parashos P, Messer HH (2008) The technical quality of nonsurgical root canal treatment performed by a selected cohort of Australian endodontists. International Endodontic Journal 41, 561–70.
Boltacz-RzepkowskaE,PawlickaH (2003)Radiographicfeatures and outcome of root canal treatment carried out in the Lodz region of Poland. International Endodontic Journal 36, 27–32.
Boucher Y, Matossian L, Rilliard F, Machtou P (2002) Radiographic evaluation of the prevalence and technical quality of root canal treatment in a French subpopulation. International Endodontic Journal 35, 229–38.
Buckley M, Spangberg LSW (1995) The prevalence and technical quality of endodontic treatment in an American subpopulation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 79, 92–100.
Chen CY, Hasselgren G, Serman N, Elkind MS, Desvarieux M, Engebretson SP (2007) Prevalence and quality of endodontic treatment in the Northern Manhattan elderly. Journal of Endodontics 33, 230–4.
Cheung GS, Liu CS (2009) A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. Journal of Endodontics 35, 938–43.
Chueh LH, Chen SC, Lee CM et al. (2003) Technical quality of root canal treatment in Taiwan. International Endodontic Journal 36, 416–22. Chugal NM, Clive JM, Spangberg LSW (2003) Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 96, 81–90.
Crump MC, Natkin E (1970) Relationship of broken root canal instruments to endodontic case prognosis: a clinical investigation. Journal of American Denal Association 80, 1341–7.
De Moor RJ, Hommez GM, De Boever JG, Delme KI, Martens GE (2000) Periapical health related to the quality of root canal treatment in a Belgian population. International Endodontic Journal 33, 113–20.
Eleftheriadis G, Lambrianidis T (2005) Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. International Endodontic Journal 38, 725–34.
Er O, Sagsen B, Maden M, Cinar S, Kahraman Y (2006) Radiographic technical quality of root fillings performed by dental students in Turkey. International Endodontic Journal 39, 867–72.
European Society of Endodontology (1994) Consensus report of the European Society of Endodontology on quality guidelines for endodontic treatment. International Endodontic Journal 27, 115–24.
European Society of Endodontology (2001) Undergraduate curriculum guidelines for Endodontology. International Endodontic Journal 34, 574–80.
Gambarini G (1999) Shaping and cleaning the root canal system. A scaning electron microscopic evaluation of a new instrumentation and irrigation technique. Journal of Endodontics 25, 800–3.
Georgopoulou M, Spanaki-Voreadi A, Pantazis N, Kontakiotis E (2005) Frequency and distribution of root filled teeth and apical periodontitis in a Greek population. International Endodontic Journal 38, 105–11.
Georig A, Neaverth E (1987) A simplified look at the buccal object rule in endodontics. Journal of Endodontics 13, 570–2.
Greene KJ, Krell KV (1990) Clinical factors associated with ledged canals in maxillary and mandibular molars. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 70, 490–7.
Hayes SJ, Gibson M, Hammond M, Bryant ST, Dummer PMH (2001) An audit of root canal treatment performed by undergraduate students. International Endodontic Journal 34, 501–5.
Helminen SE, Vehkalahti M, Kerosuo E, Murtomaa H (2000) Quality evaluation of process of root canal treatments performed on young adults in Finnish public oral health service. Journal of Dentistry 28, 227–32.
Hill EE, Rubel BS (2008) Do dental educators need to improve their approach to teaching rubber dam use? Journal of Dental Education 72, 1177–81.
Jimenez-Pinzon A, Segura-Egea JJ, Poyato-Ferrera M, VelascoOrtega E, Rıos-Santos JV (2004) Prevalence of apical periodontitis and frequency of root filled teeth in an adult Spanish population. International Endodontic Journal 37, 167–73.
Kapalas A, Lambrianidis T (2000) Factors associated with root canal ledging during nstrumentation. Endodontics and Dental Traumatology 16, 229–31.
Kfir A, Rosenberg E, Zuckerman O, Tamse A, Fuss Z (2004) Comparison of procedural errors resulting during root canal preparations completed by senior dental students in patients using an ‘8-step method’ versus ‘serial step-back technique’. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 97, 745–8.
Kirkevang LL, Horsted-Bindslev P, Ørstavik D, Wenzel A (2001) A comparison of the quality of root canal treatment in two Danish subpopulations examined 1974-75 and 1997-98. International Endodontic Journal 34, 607–12.
Lambrianidis T (2001) Risk Management in root canal treatment, 1st edn. Thessaloniki: University Studio Press. Loftus JJ, keating AP, McCartan BE (2005) Periapical status and quality of endodontic treatment in an adult Irish population. International Endodontic Journal 38, 81–6.
Lynch CD, Burke FM (2006) Quality of root canal fillings performed by undergraduate dental students on singlerooted teeth. European Journal of Dental Education 10, 67–72.
Moussa-Badran S, Roy B, Bessart du Parc AS, Bruyant M, Lefevre B, Maurin JC (2008) Technical quality of root fillings performed by dental students at the dental teaching centre in Reims, France. International Endodontic Journal 41, 679– 84.
Ng Y-L, Mann V, Rahbaran S, Lewsey J, Gulabivala K (2008) Outcome of primary root canal treatment: systematic review of the literature – Part 2 Influence of clinical factors. International Endodontic Journal 41, 6–31.
Peters OA (2004) Current challenges and concepts in the preparation of root canal systems: a review. Journal of Endodontics 30, 559–67.
Petersson K, Olsson H, So¨derstro¨m C, Fouilloux I, Jegat N, Le´vy G (2002) Undergraduate education in endodontology at two European dental schools. A comparison between the Faculty of Odontology, Malmo¨ University, Malmo¨, Sweden and Faculty of Odontology, Paris 5 University (Rene´ Descartes), France. European Journal of Dental Education 6, 176–81.
Qualtrough AJE, Dummer PMH (1997) Undergraduate endodontic teaching in the United Kngdom: an update. International Endodontic Journal 30, 234–40.
Qualtrough A, Whitworth J, Dummer P (1999) Preclinical endodontology: an international comparison. International Endodontic Journal 32, 406–14.
Ridell K, Petersson A, Matsson L, Mejare I (2006) Periapical status and technical quality of root filled teeth in Swedish adolescents and young adults: a retrospective study. Acta Odontontologica Scandinavia 64, 104–10.
Saunders WP, Saunders EM, Sadiq J, Cruickshank E (1997) Technical standard of root canal treatment in an adult Scottish sub-population. British Dental Journal 182, 382–6.
Segura-Egea JJ, Jime nez-Pinzo A, Poyato-Ferrera M, VelascoOrtega E, Rıos-Santos JV (2004) Periapical status and quality of root fillings and coronal restorations in an adult Spanish population. International Endodontic Journal 37, 525–30.
Siqueira JF Jr, Roˆc¸as IN, Alves FR, Campos LC (2005) Periradicular status related to the quality of coronal restorations and root canal fillings in a Brazilian population. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontics 100, 369–74.
Sonntag D, Barwald R, Hulsmann M, Stachniss V (2008) Preclinical endodontics: a survey amongst German dental schools. International Endodontic Journal 41, 863–8.
Stewardson DA (2001) Endodontic standards in general dental practice–a survey in Birmingham, Part I. The European Journal of Prosthodontics and Restorative Dentistry 9, 107–12.
Stewardson DA (2002) Endodontics and new graduates: part I, Practice vs training. The European Journal of Prosthodontics and Restorative Dentistry 10, 131–7.
Sunay H, Tanalp J, Dikbas I, Bayirli G (2007) Cross-sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. International Endodontic Journal 40, 139–45.
Toure´ B, Kane AW, Sarr M, Ngom CT, Boucher Y (2008) Prevalence and technical quality of root fillings in Dakar, Senegal. International Endodontic Journal 41, 41–9.
Weiger R, Hitzler S, Hermle G, Lost C (1997) Periapical status, quality of root canal fillings and estimated endodontic treatment needs in an urban German population. Endodontics and Dental Traumatology 13, 69–74.
Radiographic_quality_of_root_fillings.pdf

Σχόλια